Some basic self-care techniques for Trigger Points
Repeat after me: STOP rolling around on hard balls and ‘smashing your tissue’.
This creates unnecessary inflammation that can promote/prolong the trigger point.
Instead, find the most painful spot and use a tennis ball (or similar that is firm, yet has some give) and use a comfortable pressure i.e. bodyweight or partial bodyweight for between 30 seconds up to a maximum of 2 minutes, or until you feel a ‘release’. Try and stay still, don’t roll around.
All that is required is enough compression to deprive the tissue of oxygen. This triggers a biochemical cascade that will result in the fascicles (subunits of muscle fibres) relaxing. Rolling around and ‘smashing yourself’ on a hard ball) can have the opposite effect by creating a ‘forward feedback loop’ (small peptide molecules called cytokines may be released, which promotes inflammation, and have been shown to be part of the process in forming MTPs) as well as triggering nociceptors (pain receptors) which may also lead to the formation of MTPs.
If this isn’t enough to completely resolve the MTP, and this is often the case when they are substantial and/or long standing, this likely requires treatment – come and see me! If they resolve, but keep coming back, they are likely part of a compensation pattern in your body (overactivity in some muscles compensating for weakness in others) – come and see me!
Key Points
- Travell first coined the term ‘myofascial trigger point’ (MTP) in 1950 &, in 1983 with Simons, published the book: Myofascial Pain: the Trigger Point Manual
- Diagnosis requires at least 2 of:
- a taut band
- a hypersensitive spot
- &/or referred pain
- MTPs are a sustained contraction of muscle fascicles that constrict local circulation
- MTPs result from
- acute injury
- or sustained, repetitive muscle contraction
- e.g. an overuse injury and/or poor posture
- Small MTPs may self-resolve; however, larger MTPs may persist for months or years
- MTPs can cause pain, limit range of motion & muscle strength; can cause certain types of headaches, neck & back pain; & may lead to myofascial pain syndrome
- Best treated with ischemic pressure (i.e. thumb, elbow, etc), dry needling (particularly if larger or more painful), or other manual therapy techniques
A brief history and definition:
As far back as 1816 the British physician, Balfour, wrote about pain associated with thickenings and nodules in muscles, but it wasn’t until 1950 that Travell and Rinzler first coined the term ‘Myofascial Trigger Point’(MTP) (1). In 1983, Travell with her colleague Simons, wrote what is considered to be the seminal work on the subject: Myofascial Pain: the Trigger Point Manual, Volume A & B, which defined a MTP as ‘a highly irritable, localised spot of exquisite tenderness in a nodule in a palpable band of taut muscle tissue’ (2). Later definitions have expanded this to include ‘a taut band of skeletal muscle tissue or in the muscle fascia which is painful on compression and can give rise to characteristic referred pain, motor dysfunction, and autonomic phenomena’(3).
Diagnostic criteria
While most clinicians and researchers agree that MTPs exist, there has been a lot of debate over their diagnostic criteria. Recently, a DELPHI study (a large formal survey of experts – in this case over 60 from 12 countries) published the following guideline criteria:
Two out of three of the following – (i) a taut band; (ii) a hypersensitive spot; and (iii) referred pain.
The DELPHI study also differentiated an ‘active MTP’ – a continually painful MTP – from a ‘latent MTP’ – a MTP that is only painful when stimulated. The study also broadened the term ‘referred pain’ (in relation to MTPs) to include different sensations such as tingling, burning, spreading, etc. in addition to frank pain (4).
So, what are MTPs?
Ultrasound and thermal imaging have shown that the area of a MTP includes a ‘hotspot’ surrounded by a cool area, with the heat likely resulting from the contraction of fascicles (subunits of a muscle fibre), with the surrounding cool area due to lack of blood supply to the area (5).
So, what causes Trigger Points?
The triggering event is generally either an acute injury or sustained, repeated muscle contraction (particularly submaximal loads) where normal recovery has been disturbed. The common denominator appears to be local ischemia (lack of blood supply) and lowered pH (acidity) in the muscle tissue. Whether this is due to inflammation (from overuse, etc.) or due to nociceptive inputs (pain due to tissue damage as opposed to, say, nerve irritation) is still being debated (6).
In plain English, it’s due to an acute injury or chronic overuse such as a repetitive task, or prolonged periods of poor posture, and your body’s response has been to keep a small part of the muscle contracted, limiting blood supply.
Will Trigger Points go away and can they cause problems?
Sometimes, if they are small and not very painful, they can self-resolve. However, particularly if they are more painful, or larger in size, they can hang around for months or even years. Without diving too deep down the rabbit hole, a combination of the acidic environment and the lack of oxygen (and the reactive oxygen byproducts) can cause a forward feedback loop (continual stimulation causes more acidity and lack of oxygen in the tissues) which affects the ligand gates of the nociceptors (the pain receptors) (7). It should be noted that MTPs are particularly prevalent in certain types of headaches and are thought to be responsible in myofascial pain syndrome (6).
So, what can we do about Trigger Points?
Patients with MTPs will benefit from a multimodal treatment plan including dry needling and manual therapy techniques (8,9). Comparisons of dry needling and manual therapy techniques (ischemic pressure) have found that both are equally effective (10).
My thoughts
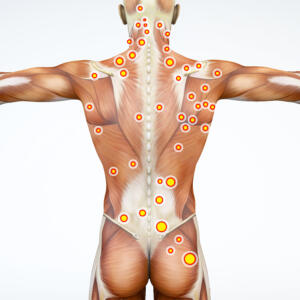
Trigger points are very common, and I often find them in the musculature of the neck and shoulders, lower back, and gluteal complex. They are often part of what we term Upper and Lower Body Postural Dysfunction syndromes.
If they are minor, simple ischemic pressure (i.e. thumb, palm or a broad elbow surface) will often be enough to relieve them (and after reading this article, you’re probably realising that I do this in most treatments). If the trigger points are very painful and/or chronic, then dry needling tends to be my ‘weapon of choice’, and sometimes I’ll get out the vibrating massage gun (although it is not as specific as dry needling).
Like a lot of painful conditions, MTPs are often the symptom and not the cause – particularly in long standing postural conditions, a longer-term fix will require strengthening the under active areas, in addition to resolving the MTPs and stretching/mobilising the overactive areas.
References
- Vázquez Delgado E, Cascos Romero J, Gay Escoda C. Myofascial pain syndrome associated with trigger points: A literature review. (I): Epidemiology, clinical treatment and etiopathogeny. Med Oral Patol Oral Cir Bucal. 2009;14(10):494–8.
- Simons DG, Travell JG, Simons LS. Travell & Simons’ myofascial pain and dysfunction : the trigger point manual. 2nd ed. Myofascial pain and dysfunction. Baltimore: Williams & Wilkins; 1999.
- Lavelle, E. D., Lavelle, W., & Smith HS. Myofascial trigger points. Anesthesiol Clin [Internet]. 2007;25(4):841–iii. Available from: https://doi.org/10.1016/j.anclin.2007.07.003
- Fernández-de-las-Peñas C, Dommerholt J. International consensus on diagnostic criteria and clinical considerations of myofascial trigger points: A delphi study. Pain Med (United States). 2018;19(1):142–50.
- Cojocaru MC, Cojocaru IM, Voiculescu VM, Cojan-Carlea NA, Dumitru VL, Berteanu M. Trigger points–ultrasound and thermal findings. J Med Life. 2015;8(3):315–8.
- Bron C, Dommerholt JD. Etiology of myofascial trigger points. Curr Pain Headache Rep. 2012;16(5):439–44.
- Jafri MS. Mechanisms of Myofascial Pain. Int Sch Res Not. 2014;2014:1–16.
- Money S. Pathophysiology of Trigger Points in Myofascial Pain Syndrome. J Pain Palliat Care Pharmacother. 2017 Jun;31(2):158–9.
- Barbero M, Schneebeli A, Koetsier E, Maino P. Myofascial pain syndrome and trigger points: evaluation and treatment in patientswith musculoskeletal pain. Curr Opin Support Palliat Care. 2019 Sep;13(3):270–6.
- Lew J, Kim J, Nair P. Comparison of dry needling and trigger point manual therapy in patients with neckand upper back myofascial pain syndrome: a systematic review and meta-analysis. J Man Manip Ther. 2021 Jun;29(3):136–46.